
Case
D. is a young adult living at home with his parents. For the past year or so, he stays up until 12 AM or later. He wakes up around 8 AM, tired and exhausted. Parents try their best to ensure there are no screens past 9 PM, but nonetheless, he is simply unable to fall asleep earlier.
By 11 PM, it is as if he gets a “second wind,” at which point he doesn’t feel like sleeping. He finally falls asleep past midnight but then struggles to get up at 8 AM for school, even with multiple alarms and parents’ nagging.
Terms
Note that DSPD was previously known as delayed sleep phase disorder, now renamed to delayed sleep-wake phase disorder, in order to emphasize the significant problems caused during waking hours when one is unable to sleep.
What is Delayed Sleep-Wake Phase Disorder (DSWPD)?
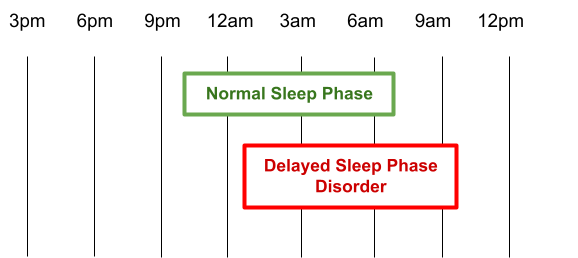
DSWPD is a sleep disorder characterized by a discrepancy between one’s circadian clock’s internal setting and the sleep wake schedule required by one’s occupational, educational or social obligations.
The sleep disruption leads to fatigue and/or insomnia and produces clinically significant distress or impairs one’s social, educational or occupational functioning (American Psychiatric Association, 2013).
When the person tries to sleep like everyone else (e.g. go to bed at 11 PM, wake up at 7 AM), their sleep quality is very poor, however they have significant improvements in their sleep architecture and continuity when allowed to go to bed and wake up later.
Normal Sleep Physiology
The timing of sleep is controlled by the master circadian clock, located within the suprachiasmatic nucleus.
It is this clock that determines what time to go to sleep, what time we wake up.
Our clock requires constant “resetting” by external time cues (aka “zeitgebers”), and the most important ones that set our clock include exposure to sunlight during the morning and daytime; physical activity, body temperature, meals; exposure to darkness in the evening.
Epidemiology
Most common in adolescents (0.4-4%) (Siverson, 2013).
Clinical Presentation
Features
- The person has trouble getting to bed on time and thus has trouble waking up for obligations such as school or work.
- The person feels most alert, productive and creative late at night.
- If forced to get up early, the person is tired and sleepy during the day.
- Others may perceive the person as unmotivated and lazy because they are late for morning responsibilities, e.g. late for school, work.
- When allowed to sleep at the preferred delayed sleep phase, sleep quality and duration are typically within the normal range for age.
ICSD-2 Criteria for Delayed Sleep Wake Phase Disorder (DSWPD)
According to the International Classification Sleep Disorders (ICSD-2)., diagnosis is made by history of:
- Delay of the major sleep period relative to the desired sleep and wake times for at least 1-3 months,
- Clinically significant insomnia and/or excessive sleepiness.
According to the DSM-5, delayed sleep phase type is:
- Delayed onset of sleep and poor maintenance of sleep, with an inability to fall asleep or wake at the desired time (American Psychiatric Association, 2013).
- This is more commonly seen in adolescents (Martinez, and Lenz, 2010).
Other Circadian Rhythm Sleep Disorders
Delayed sleep-wake phase disorder is a type of circadian rhythm sleep disorder. Other types of circadian rhythm sleep disorders are:
- Advanced sleep phase disorder
- Sleep onset and awakening times are advanced, and the patient is unable to stay awake or remain asleep until the desired time (American Psychiatric Association, 2013).
- People fall asleep in the early evening (6-9 PM), and wake up in the early morning (2-5 AM)
- Most often seen in the elderly (Martinez, and Lenz, 2010).
- Jet lag
- Jet lag is when people have travelled to a destination that has a significantly different time zone that their starting location.
- As a result, the person has troubles adjusting to the new sleep-wake cycle.
- Shift work disorder
- Insomnia secondary to shift work, and/or fatigue which can include falling asleep unintentionally.
- When people are frequently switching between different hours of shift work (e.g. day shifts, evening shifts, night shifts), it confuses the body’s natural circadian rhythm.
- Sleep deprivation is felt to have contributed to many disasters such as the Exxon Valdez oil tanker, the space shuttle Challenger, Chernobyl nuclear reactor meltdown, and many more.
- Irregular sleep-wake rhythm
- The sleep /wake cycle is disorganized, with variable sleep wake periods during a 24 hour period.
- People have an undefined sleep-wake cycle, often seen in those with underlying neurological issues, e.g. dementia, intellectual disabilities, traumatic brain injuries.
- Non-24-hour sleep-wake syndrome
- Persons have an internal clock which is longer than 24-hrs, and as a result, there is a daily drift of progressively later sleep onset and wake times, usually by 1-2 hrs each day.
- Usually seen in those who are blind.
Risk Factors for Circadian Rhythm Sleep Disorder
Risk factors include:
- Family history, e.g. Having a first-order relative with CRSD, is a risk factor (American Psychiatric Association, 2013).
- Poor sleep hygiene (e.g., texting or eating in bed or an irregular bedtime) can contribute to CRSD.
- Flex-time work schedule or working swing-shift can lead to CRSD
- Napping during the day or sleeping past one’s usual rising time.
Comorbidity of DSWPD
There is high comorbidity with:
- Attention deficit hyperactivity disorder (ADHD)
- Mood disorders including major depressive disorder and bipolar disorder.
- Seasonal changes: Patients frequently report seasonal changes in mood and energy.
Long-term health problems from insufficient sleep and working against one’s circadian rhythm include metabolic syndrome, obesity and diabetes.
Diagnosis of DSWPD
To make the diagnosis of DSWPD, the following is recommended (American Academy of Sleep Medicine, 2005):
- Sleep diary / logs (such as a paper diary, sleep tracking app) (actigraphy if possible) for at least 7-days
Diagnosis is confirmed by a delayed pattern of the habitual sleep and wake cycle.
Investigations
A polysomnograph or overnight sleep study can be helpful.
Management of DSWPD
Morning
- Ensure regular, consistent wake-up times.
- Consider a daylight simulator as the morning alarm clock. Consider the use of 10 000 lux lightbox for 30-60 min at desired wake time (e.g. 7 AM).
- Consider bright light therapy in the morning right after awakening (30-60 min each morning) to advance the circadian rhythm.
- Otherwise, ensure exposure to sunlight in the morning and daytime.
- Light exposure can be gradual. If the patient sleeps in until 12 PM for example, then start with light exposure at 12 PM. After that, gradually advance by 30-min. every 2-days until the desired goal wake up time is reached.
- Note: Adverse effects that have been reported include photophobia, migraine, triggering of mania in those with vulnerability to bipolar disorder
- Are there ocular diseases?
- If so, then refer for eye examination with optometrist or opthalmologist
Afternoon / dinnertime
- Low dose melatonin 0.5 mg given 6-8 hrs before sleep to advance circadian rhythm earlier by 90-120 min.
- Patient up until 12 AM? Give at 4-6 PM.
- Patient up until 2 AM? Give at 6-8 PM.
- Adjust as necessary.
Evening
- Ensure good sleep hygiene.
- Regular bedtime.
- Ensure there is a screen curfew, i.e. no screens past 8-9 PM.
- Ensure a dim light environment at night time. Eliminate any bright lights (especially blue light) before bedtime.
- In the bedroom, have a red or orange light bulb in the bedside table lamp. About 1-2 hrs before bed time, turn on the red (or orange) lightbulb.
- Alternatively, consider low blue light glasses that block blue spectrum light.
Bedtime
- Quiet, relaxing activities such as reading, drawing, writing.
- Avoid electronic activities as they can be activating due to blue light (even with ‘low blue light mode’) and due to being mentally stimulating (e.g. social media, news, etc.)
- If devices must absolutely be used, use them for audio such as music, mindfulness meditation, etc.
- Is the person still having troubles despite above strategies?
- If so, then melatonin 3-5 mg bedtime at 30-60-min. before bedtime, followed by dim environment.
Melatonin
Dosage
- Melatonin at low doses (0.3-1 mg) 6-8 hrs before bedtime to advance the sleep phase.
- Melatonin at higher doses (3-10 mg) produces hypnotic effects (as opposed to advancing circadian rhythm), and is usually given 30-60-min. before bedtime.
- Headaches
- Sedation
- Hypotension
- Nightmares
- Daytime sedation.
Caution and monitor closely with the following populations:
- Children
- Adolescents with delayed puberty
- Women of reproductive age
- Patients with depression or epilepsy
- Patients on warfarin
Treatment with Comorbid ADHD
Does the patient have comorbid ADHD?
Studies have confirmed the use of melatonin in treating children with comorbid ADHD, though there is a rare adverse effect of new onset seizures (Smits, 2001).
Societal and Policy Interventions
Given the high rate of sleep phase delay in adolescents, there are school districts that have accommodated this by starting school at a later time.
As adults and employees, people with sleep phase delay presumably do better in occupations that accommodate a later start time, e.g. restaurant workers (in restaurants that serve lunch/dinner), self-employed individuals, evening shifts (not day shifts), etc.
Prognosis
Prognosis is good as DSPWD generally responds well to treatment.
Case, Part 2
You recommend the following:
- Low dose melatonin (0.5 mg), taken 5-hrs before bedtime in order to advance his circadian system
- Bright light exposure in the morning, starting as his wake up time, and progressively advancing by 30-min. every few days
- Putting his electronics away by 9 PM. Unfortunately, he has resistance to putting away his electronics, so instead you recommend that he wear orange colored glasses (i.e. low blue light) as well as replce his normal full-spectrum night table light with a red light (i.e. low blue light) in his bedroom.
You see him a few weeks later and he reports improvement in his sleep wake cycle.
When and Where to Refer
For patients with delayed sleep-wake phase disorder that do not respond, consider referral to a sleep specialist.
Practice Guidelines
2015 American Academy of Sleep Medicine (AASM) Practice Guidelines for the Treatment of Circadian Rhythm Sleep-Wake Disorders
References
American Academy of Sleep Medicine . The international classification of sleep disorders: diagnostic & coding manual. 2nd ed. American Academy of Sleep Medicine; Westchester, IL: 2005.
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders. (5th Edition). Washington, DC.
Boivin D: Treating delayed sleep-wake phase disorder in young adults, J. Psychiatr. & Neuroscience, Sep 2017, 42(5): 360.
Ohayon MM, Roberts RE, Zulley J, Smirne S, Priest RG. Prevalence and patterns of problematic sleep among older adolescents. J Am Acad Child Adolesc Psychiatry. 2000 Dec;39(12):1549-56. doi: 10.1097/00004583-200012000-00019. PMID: 11128333.
https://pubmed.ncbi.nlm.nih.go...
Sivertsen, B., Pallesen, S., Stormark, K.M. et al. Delayed sleep phase syndrome in adolescents: prevalence and correlates in a large population based study. BMC Public Health 13, 1163 (2013). https://doi.org/10.1186/1471-2...
Smits MG, Nagtegaal EE, van der Heijden J, et al. Melatonin for chronic sleep onset insomnia in children: a randomized placebo-controlled trial. J Child Neurol. 2001;16:86–92. [PubMed]
About this Document
Written by Dr’s Elliott Lee, FRCP(C), Psychiatrist, Royal Ottawa, uOttawa; Dr's Michael Cheng, FRCP(C), Psychiatrist, CHEO, uOttawa; Dhiraj Aggarwal, Psychiatrist, CHEO, uOttawa.
Conflicts of Interest: No competing interests declared.
Disclaimer
This information is offered ‘as is' and is meant only to provide general information that supplements, but does not replace the information from a qualified expert or health professional. Always contact a qualified expert or health professional for further information in your specific situation or circumstance.
Creative Commons License
You are free to copy and distribute this material in its entirety as long as 1) this material is not used in any way that suggests we endorse you or your use of the material, 2) this material is not used for commercial purposes (non-commercial), 3) this material is not altered in any way (no derivative works). View full license at https://creativecommons.org/licenses/by-nc-nd/4.0/
 Printing This For Someone?
Printing This For Someone?



